
Note: This is a rough transcript of episode 14 of Health Savings News and has been lightly edited for clarity. Copy may not be in its final form.
[Fundraising appeal]
[intro music] (2:09)
Evan (2:19):
Hello, and welcome to Health Savings News: the podcast about healthcare costs in America and how to save money on the often expensive care all kinds of people need. I’m your host, Evan O’Connor, joined by retired doctors, Rich Sagall and Mike Woods. Each episode we discuss healthcare costs in America, offer tips for saving money, and relevant news that affects and reflects the expensive landscape of healthcare in America. This week’s topic is a continuation of last week’s on why healthcare costs so much. Last time, we discussed the systemic reasons for expensive healthcare in the United States, and this week we’ll be talking about the medical reasons that affect healthcare costs.
Rich (02:51):
Well, I think it’s important to remember that prevention is better than any treatment, so we want to emphasize that. Non-adherence is also a problem, which is not following a treatment plan. The reason you have a treatment plan is to control problems and that helps to control cost by keeping down unnecessary and emergency medical care. Non-compliance can fall into a couple of categories. One is just not taking the pills or doing the treatments. Another is inability to comply with the treatment plan. Maybe it’s due to financial reasons or personal reasons, or the treatment plan is overly complex. Chronic diseases such as cancer, cardiovascular disease, diabetes, and COPD (or chronic obstructive pulmonary disease) are responsible for most of the deaths and healthcare costs in this country. It’s estimated that the sickest 5% of our population generate 50% of the total healthcare costs, and the healthiest 50% generate only 3%. Another aspect of keeping healthcare costs down is lifestyle choices. There are many things that we do in this country that cause preventable diseases, and this includes obesity, smoking, substance abuse, poor oral hygiene and environmental damages resulting in exposure such as air pollution, increased radiation from the sun, excessive heat, tainted water, toxic waste or spills. While chronic diseases such as cardiovascular disease and diabetes continue to increase in frequency, much of this could have been prevented with lifestyle changes in early diagnosis and treatment. We can talk about poor eating habits, and this can be due to choice or to poor access. We talk about food deserts, which refer to the inability to find healthy foods at reasonable prices and grocery stores are too far away to be convenient. It’s estimated that over 23 million Americans live in what are called food deserts in this country, nearly half of whom are low income.
Evan (04:54):
When we talk about lifestyle choices and access to food and eating habits, we’re really talking about the social determinants of health. Housing, clean air, clean water, public sanitation, social supports — these are all parts of healthcare that are not always addressed.
Mike (05:14):
Well, speaking of prevention, let’s talk about vaccines. Vaccines have been one of the biggest success stories in medicine. Over the past century we have significantly reduced a large number of many devastating infections. The problem is the fact that most of these diseases — maybe with the exception of a smallpox — have not disappeared. So this current trend of vaccine hesitancy in refusal has resulted increasing the number of otherwise preventable infections that the scientists have worked so hard over the years to suppress. The most well known, and we’ve talked about it in the past, is measles. The reduction in measles vaccination was associated with a fabricated report of an association of the MMR vaccine with autism spectrum disorder. Unfortunately, now that these findings have been negated, it has not changed many people’s minds about the MMR vaccine. There are examples in adults that are very preventable diseases, including shingles and pneumococcus. I was a practicing pediatrician in about 20 years ago, I remember we had a whooping cough epidemic in our nursery. We eventually figured out that the infants were catching it from adults whose pertussis immunity had worn off over time, and adding pertussis to the current adult tetanus and diptheria boosters resolve the issue. Today, the most current examples are influenza and COVID-19. Because of vaccine hesitancy and refusal each year, many people get and die from influenza because of their lack of vaccination. for the COVID-19 infection, this says produced a lot of significant results including pro prolongation of the pandemic, more people with COVID disease that would otherwise have avoided it, a huge financial burden on healthcare costs, a detrimental effect on our in the world’s economy, such as the current inflation rate. In addition, there’s been millions of unused COVID vaccination doses that have wasted enormous amount of money. To summarize, to help fight this it’s important to remember that although vaccines are not without risk and they don’t always work, the side effects are much milder than the disease and the complications of the disease itself, and that the anxiety and fear that has resulted in reduced vaccination rates are often due to exaggerated or sensationalized reports by the anti-vaxxers.
Rich (07:48):
One important way to keep medical costs down is appropriate medical screening for diseases, and the screening contributes to saving costs in two ways. Not screening is a missed opportunity and to catch a disease at an early stage where treatment makes the most difference and the diseases instead present later on when they’re more severe, more costly, and have more complications. Screening may not be as effective for those without risk factors. Screening and providing preventive treatment for large numbers of people to prevent a few from developing disease can needlessly increase the cost of preventive care. The cost effectiveness and likelihood of the benefit of screening are being considered before implementing them. Although some habits are hard to break even in the medical world when presented with evidence, we need to reevaluate the value of some screening tests
Mike (08:34):
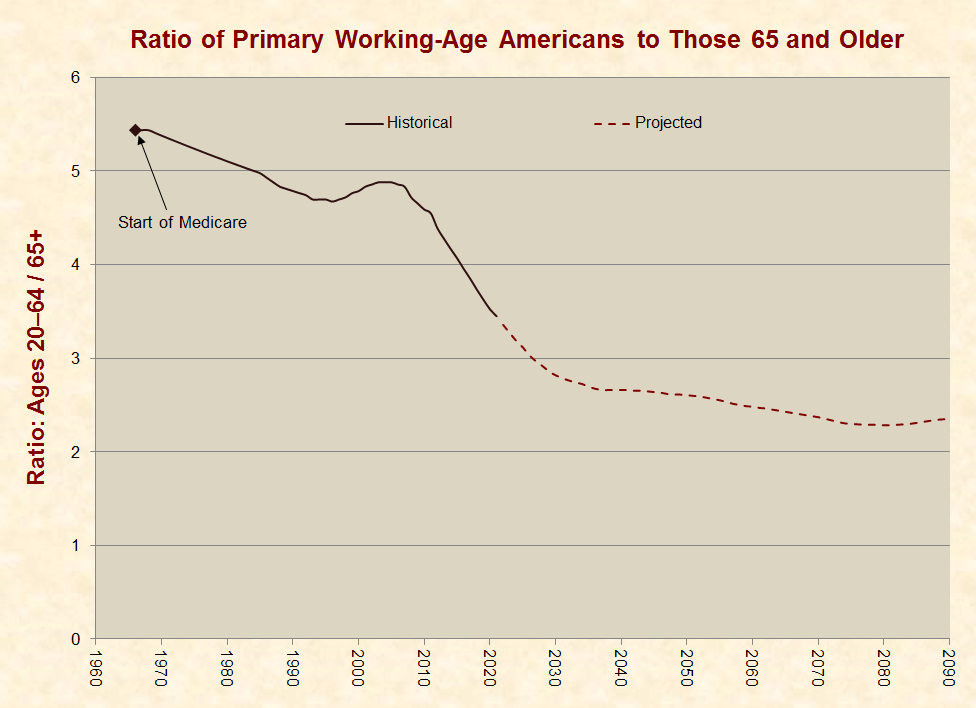
Over time, another major cost of increased medical care is population changes. We’ve already talked about the fact that there are now more people with chronic conditions and severe diseases as a result of the issues that Rich has already discussed. However, another thing that we can’t avoid is that we have an aging population. Now, medical care improves over time and people live longer and they need medical care for a longer amount of time, and over time the amount of conditions that each person has increases. So an elderly person will have many more individual medical conditions than a young and healthy person. As a matter of fact, adults over 65 and especially those over 85 have five times higher medical expenses than children and almost three times more health expenses than working age people. Elderly and people with chronic diseases are more likely to need emergency room treatments and hospitalizations. They often have trouble affording medications, which starts the vicious cycle that results in both more health problems, more ER visits, and higher medical costs. The aging baby boomer generation has also resulted in a lower ratio of working age people to retirement age citizens. Currently it’s about 3.5/1, but that ratio is decreasing over time, meaning that as time goes on, more people will be on Medicare and more people will be on social security over time as the amount of people paying taxes to SU support part of these programs decreases. COVID has produced a lot of unemployment over time, and from that, a lot more people with low income who now will need Medicaid or other premium assistance programs for medical health.
Evan (10:20):
I would say more than unemployment, COVID also has added to people unable to work either through disability or chronic health that has come from their COVID infections.
Mike (10:32):
Another one that is very commonly seen as overuse of medical services, and in a lot of cases especially emergency rooms. While emergency rooms are crucial for care, critically ill patients and those with urgent medical needs, they are used for an entire gamut of medical care — including a lot of care traditionally done by primary care providers. Although this may be the only option for those without insurance, since people know emergency rooms are required to care for patients regardless of their ability to pay. However, for those who could have seen a less expensive option, emergency rooms are very expensive for routine problems. Patients pay both provider fees and all of the ER costs. Emergency room providers tend to order more tests because they often lack the ability to follow up patients to see how they’ve done on the treatments. For the same reason, they often provide unnecessary care. And although most insurance companies do charge higher copays for emergency care and pay less, if the care was not emergent or an emergency, it really doesn’t off set the extra cost. In fact, unnecessary ER visits can cost up to $32 billion a year. This all cycles back to the policy holders in the form of higher premiums, higher contributions to employee sponsored health insurance, and/or higher out of pocket expenses such as deductibles and copays. A lot of this money spent in ERs could have been avoided if patients took better care of themselves, as we’ve previously discussed. Other contributors to the unnecessary visits include those that are for trivial problems or ones that could have been resolved with a phone call. There’s also a lot of unnecessary and inappropriate visits to specialists for reasons such as not trusting their primary care doctor to have the knowledge to take care of that particular problem, pressure from friends or others that insist that they see a specialist for their problem. Medical care is done by humans. So doctors like us were prone to error, excess, and waste from medical errors, inappropriate, unnecessary and out-of-network medical care to unused medications and medical supplies. That adds up to about 25% of the total medical spending.
Rich (12:57):
We also need to look at errors in what we call low value care. Medical and medication errors are detrimental in terms of human suffering and can be financially costly. It was estimated in 2019 the impact of medical errors and medication errors was over $600 million — that’s just in Massachusetts. More costly is that 86% of mistakes are made in the healthcare industry are administrative and can cost over $216 billion. Another thing to look at is unnecessary and low value testing and treatment. When we say low value, these are tests that don’t contribute to treatment decisions such as follow up imaging, routine labs at annual checkups, et cetera. Tests are easy to misinterpret. A rapid strep screen without a clinical suspicion may give a positive result that’s not– does not indicate an infection. Random urinalysis gen rarely shows any significant problems. Another issue is overtreatment. This is care with little to no benefit to the patients such as treating self-limiting conditions or over-prescribing antibiotics.
Mike (14:02):
Like any other industry and things in life, there’s a lot of waste that happens in medicine that includes waste, waste of resources, supplies and time. A lot of the causes of waste include the administrative complexity. So as with healthcare insurance, a lot of administrative costs are due to the necessity of more employees to handle the increasingly complex system that we’ve talked about in the past. And this can result in over $250 billion of wasted money. There is occasionally some inadvertent or even deliberate overcharging of patients that healthcare providers and testing facilities can get away with, and that can amount to about the same amount at about $230-240 billion a year. People missing appointments isn’t as innocuous as it would seem from a financial point of view, and in fact, $150 billion a year is wasted on time and resources that need to be spent for missed appointments. Staff have to track down patients who missed appointments, notify them and spend time rescheduling the appointments. There are missed opportunities for preventive care or reducing the severity of disease that could have prevented medical problems in the future. And there’s also having to pay salary for staff that have less to do when patients don’t come to the office. There is ineffective care that’s similar to what we’ve talked about as low value care, but in this case, it’s injuries and worse clinical outcomes due to providers using outdated or ineffectual treatments, which can result in almost a hundred billion dollars of year excess, or poor execution or lack of widespread adoption of the best clinical care practice such as the preventative care practices and screening we now know are effective, patient safety issues such as condoning, stopping smoking, wearing seatbelts, helmets on bikes and things like that. So if the provider spent more time on these sort of preventive activities, we might be able to save up to $165 billion a year.
Rich (16:07):
Another issue is unused medications. It’s estimated that 67% of all prescriptions go unused, and there are a number of reasons for this. The patient may just stop taking the medication. The prescriber may give more medication than is needed. The medicine may expire before it can be used. Patients will often stock power medication to have it just in case they need it later on. Lost medication, unneeded refills, and too many medications to take for the patient to take them properly. Another problem is taking unnecessary medications. We’re talking about coughing cold medications, for example, pain meds for very little small aches or small pains, antibiotics for viral infections. It’s estimated that $10 billion of unused over the counter medications are incinerated every year. This doesn’t even account for all the medications sitting unused and usually expired in medicine cabinets or thrown out. And we haven’t taken into account the use of supplements, homeopathic medicine, and other unproven treatments.
Mike (17:12):
Yeah, speaking of waste, we produce more medical waste than any other country in the world. Annually we produce about 3.5 million tons of medical waste at an average disposal cost of $790 per ton. So this total’s about another $2.8 billion added to medical costs. And unfortunately again, as Rich mentioned above, a lot of this waste is unused. Much of this is due to a process called bundling. It’s especially seen during surgical and other procedures where a sterile package containing anything that could possibly be used for that specific procedure, all in one sterile package, usually at the request of the provider during the procedure only some of these supplies are used in the unused ones are are thrown out or needing to have the expensive process of sterilization done on them for them to be used the next time around. Some of the most common things are sponges, blue towels and gloves, but sometimes even a one-time use attachments to instruments and medical devices go unused and are thrown out. There’s also, like medications, there’s also a lot of unused medical supplies that get thrown out that are either discarded because they’ve passed their expiration date or replaced with updated ones, and the hospitals spend a lot of money keeping track of this and doing this. When you’re in the hospital, you get a package for your room that may include a urinal, a cup, stuff like that. And most of the time they’re never even opened cuz most patients don’t really need a bed pan. Despite that, all this unused stuff is thrown out over the years. Uncoordinated medical care and miscommunication also contributes significantly to the excessive cost of medication. So this is for communication between medical or healthcare providers, medical systems, insurance companies and hospitals. This results in over $78 billion a year in excess costs. A lot of this miscommunication results in fragmented and disjointed care, such as redundant services, testing and treatment,un necessary hospital readmissions when the inpatient doctor doesn’t communicate with the outpatient doctor to continue a treatment plan out of the hospital. It also results in avoidable complications, declines in functional status and, and otherwise adverse effects for those that are chronically ill. Even if you are missing a chart or lack the appropriate information at the time of a visit or an admission, which happens in up to 30% of visit, that has the same effect the medical people have to go over your history again, fill in all the missing information from the chart, which takes time, and obviously a lot of extra money. About 80% of all serious medical errors in approximately 20% of all malpractice claims involve a specific type of miscommunication between healthcare providers called handoff communication. This is where two providers transmit information about a patient they are taking care of to the new doctor who will now be taking over the care of that patient. Mostly it happens in a hospitalist situation where a different hospitalist has finished his coverage for the week and is now passing on all of his patients to the new provider. Now that’s a lot of information and it’s not difficult to imagine that they’re not gonna get all the, the nuances and important information in the time is spent handing off. But it also happens in the handoff of patients from in patient providers to the primary care or of the primary care person to the facility that they are admitting them to. So a lot of this results in patient harms, delays in treatment, inappropriate treatment, increased lengths of stay in a hospital and a lot of wasted time giving medical history and information list to multiple providers.
Rich (21:24):
Another problem is what we call futile medical care. This is when care is given and it’s not going to affect the outcome. Some examples are resuscitation efforts when the chances of revival are negligible, such as when someone dies at home without advance care directives or do not resuscitate order with unwitnessed cardiac arrest. Another example is patients who are put on life prolonging treatment with little and no chance of recovery. They have a terminal illness such as end stage cancer and further treatment may not extend their life, or if it does, it’s by a small amount. Another issue we have to deal with is newly developed technologies and cutting edge care. Although medical devices account for 2% of healthcare spending in 2019, new or increased use of medical technology contributes a much larger share to the increasing cost of medical care. New high tech treatments are being developed to help patients better control chronic diseases such as diabetes. There are lots of good treatments, but often we don’t know when to use them, and so we use them on everybody. These new treatments are often very expensive and may not have clear cut benefits over traditional treatments. This is especially true with unnecessary features. For example, there is a more expensive glucose monitor that talks to people with diabetes. Although it makes sense for those who have developed visual impairment, it may not be necessary for those who can see normally. The higher cost includes all the accessories you might need for something new, such as special batteries, custom connectors and tubing, probes, sensors, wifi, bluetooths, a smartphone, necessary software updates, and replacements when things wear out. Many new high tech testing methods are also being developed. This occurs when new treatments may not have an advantage over traditional or less expensive methods. There also may be methods that do not replace older methods, but are used in addition to them. It may not be necessary. And while many reveal additional details, in many cases, the details may inform healthcare professionals without resulting in any change in treatment. We use high tech medical instruments and other medical technologies more often than in other countries. Like pharmaceutical companies, those who manufacture and supply these devices are also unregulated and make generous profits from the devices they sell. In many instances, there’s limited competition for these devices and this can lead to high costs which insurance companies try to negotiate to lower the costs or pass the costs on to the patient. Like pharmaceutical companies, device manufacturers spend lots of money on advertising to hospitals, healthcare providers and patients. Despite this, they typically have a margin profit of about 12%.
Mike (24:07):
The final contribution to the cost of medical care is sort of near and dear to all of us who have or are providers, and that’s malpractice and defensive medicine. Malpractice — real or perceived — contributes to a higher medical cost in several ways. In each case, the ultimate financial burden is passed on to patients. Malpractice insurers is expensive. Both healthcare facilities and healthcare providers have malpractice insurance. Most hospitals are for-profit and physicians or healthcare providers like to earn good salaries. So these costs for malpractice result in increased fees that are charged by the hospitals and the medical care providers. Medical lawsuits in of themselves are very expensive, even if malpractice didn’t occur and that the case is eventually dismissed. Although the complication, there is a legal concept for standard of care, which is defined as an acceptable degree of care and skill that the average healthcare provider who practices in that specialty is expected to give based on the medical knowledge that is currently available in the field. Despite that very nice accurate description, in court the definition of malpractice is actually somewhat arbitrary. In a lot of cases, the juries are more sympathetic toward the patient in these cases, and the arbitrariness of that allows that to happen. You can see if you follow graphs or studies, you’ll see that when the amount of malpractice settlements go up, the cost of medical care goes up with it. Even frivolous lawsuits contribute to this. Malpractice is a very complicated subject and it’s continuing to evolve, so it’s nothing we can get into in detail in here, but the future may hold the development of specific guidelines for medical care that will bring consistency to the legal aspects of malpractice. However, this still won’t address any of the unregular related or frivolous medical settlements. To a lesser degree, defensive medicine contributes to this. So theoretically the best way to avoid malpractice is to do as much as you can to prevent anyone looking to blame you for a bad medical result. So what the providers and the hospitals try to do to prevent this is to do unnecessary referrals to unnecessary testing and scans to cover all bases, including for things that are very unlikely to happen. So in many cases, this will be in order to rule out a rare or, again, unlikely condition or to appease a patient so that the provider can’t be accused of ignoring the patient’s information or of doing everything possible to rule out particular diseases. Matter of fact, three quarters of physicians do this. 21% of them actually do it on a regular basis. So it does contribute a lot. I don’t know how eventually this will resolve itself, but it really does come down to a trust issue between patients and physicians, which to me seems a little bit rocky at the moment for whatever reason.
Rich (27:32):
Well, I think that it’s a difficult issue because patients come in with certain expectations and I think it’s incumbent upon the physician to try to determine what the patient’s expectations are and address those. Good communications can lessen the need for unnecessary testing and unnecessary medications. But often the physicians and other providers don’t have enough time to really address those issues.
Mike (27:57):
Or they occasionally won’t meet somebody who’s not open to having that kind of discussion.
Rich (28:02):
That’s true.
Mike (28:05):
Despite all the information that we gave you today, we’ve really only scratched the surface of why our medical care is so expensive and we could never hope to cover all the issues. But the most important thing to remember is that it’s all complex system that our interrelated to each other, whether it’s social determinants, how doctors practice, how patients perceive medicine, how efficient we are at using resources. It’s all so complexly interrelated that it’s really difficult for any one person to understand, let alone get across in a short podcast like this one.
[segment break]
Evan (28:53):
The last segment of each episode, we suggest some of the culture, art, entertainment, and social causes we’ve been engaged with to each other and our listeners. This is the last episode we’re doing before the midterm elections, so I just want to encourage everybody to get out and vote on November 8th or early if that’s available in your area. We encourage you to support healthcare, health equity, lower healthcare costs, and all care for all people.
Thank you so much for joining us for this episode of Health Savings News. Please subscribe, rate, and review us on Apple Podcast or wherever you’re listening to the show, it really does help. You can follow @NeedyMeds on Twitter, Facebook, Instagram, LinkedIn, YouTube, and you can follow @HealthSavingPod (no S at the end of saving) on Twitter for updates specific to this podcast and send questions, comments, and topic suggestions to podcast@needymeds.org. Our music is composed by Samuel Rulon-Miller. His music can be found at musicisadirtyword.bandcamp.com. The Health Savings News podcast is produced by me, Evan O’Connor. All the sources we used in our research can be found in the episode’s podcast description on our website or your podcast app of choice. Health Savings News is not intended to substitute for professional medical, financial, or legal advice. Always seek the advice of a qualified healthcare professional, or appropriate professional with any questions. Views expressed on Health Savings News are solely those as the individuals expressing them. Any views expressed do not necessarily represent views in Health Savings News, other contributors, the NeedyMeds organization, or staff. Thanks again for listening. See you in two weeks with our next episode.
Sources:
https://www.thebalance.com/causes-of-rising-healthcare-costs-4064878
https://www.ahajournals.org/doi/pdf/10.1161/circulationaha.108.190186
https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1002578
https://www.immunize.org/catg.d/p4026.pdf
https://www.insiderintelligence.com/insights/aging-population-healthcare/
https://www.ajmc.com/view/aging-population-continuing-to-drive-national-health-spending-report-says
https://www.ajemjournal.com/article/S0735-6757(19)30300-6/fulltext
https://www.justfacts.com/images/healthcare/inverse_dependency_ratio-full.png
https://www.justfacts.com/healthcare.asp#spending-administration
https://health.costhelper.com/emergency-room.html
https://time.com/3754900/doctors-unnecessary-tests/
https://www.propublica.org/article/unnecessary-medical-care-is-more-common-than-you-think
https://getreferralmd.com/2016/08/30-healthcare-statistics-keep-hospital-executives-night/
https://jamanetwork.com/journals/jama/article-abstract/2752664
https://www.insurancejournal.com/news/national/2019/10/08/544846.htm
https://www.acsh.org/news/2019/10/08/healthcare-one-mans-waste-another-mans-income-14327
https://www.healthaffairs.org/do/10.1377/hpb20121213.959735/full/
https://getreferralmd.com/2016/08/30-healthcare-statistics-keep-hospital-executives-night/
https://pubmed.ncbi.nlm.nih.gov/24018712/
https://medlineplus.gov/ency/patientinstructions/000468.htm
https://www.thehastingscenter.org/briefingbook/health-care-costs-and-medical-technology/
https://www.healthaffairs.org/do/10.1377/hblog20200602.168241/full/
https://www.thehastingscenter.org/briefingbook/health-care-costs-and-medical-technology/
https://www.thebalance.com/why-reform-health-care-3305749
https://www.justfacts.com/healthcare.asp#_ftn713
https://www.thebalance.com/why-reform-health-care-3305749
https://www.justfacts.com/healthcare.asp#_ftn713




{kind=link}